

























Hip joint disease is a common degenerative dystrophic disease of the hip joint in which the femoral head joint and the pelvis and acetabulum are gradually destroyed due to changes in age or other factors. It is accompanied by pain and limitation of range of motion of varying severity, depending on the stage of development. If hip disease can be managed conservatively in the initial stage, then in stage 3, only by performing surgery.
It belongs to the number of joint diseases that may be accompanied by the development of similar processes in other joints, and this pathology accounts for about 12% of all diseases of the musculoskeletal system. But the term "hip disease" can only be used to describe degenerative dystrophic changes in the hip joint.
What is Hip Disease
Hip arthropathy is a complex pathology of one or both hip joints in which the layer of cartilage covering the femoral head and acetabulum is destroyed, resulting in a reduction in the size of the joint space. As the disease progresses, the appearance of deformations on the bone's surface and the formation of bone growths, called osteophytes, are observed.
Hip disease is the second most common disease of the musculoskeletal system. More commonly, only knee arthropathy, degenerative dystrophic changes in the knee joint, is diagnosed. However, hip disease has a significantly higher probability of disability.
The entire hip joint is enclosed in a specific condition called the joint capsule. It has a so-called synovial membrane, which produces synovial fluid. This fluid is essential for the proper functioning of the joint, as it not only lubricates the hyaline cartilage, but is also a source of nutrients for it.
Normally, cartilage wears down continuously and recovers immediately due to the ongoing regeneration process, which is carried out with the help of substances that enter in the synovial fluid. But with injury or age-related changes, the rate of the regeneration process decreases, which can lead to gradual wear of the hyaline cartilage and the development of hip arthropathy.
This is due to changes in the amount of synovial fluid produced and its composition. Under the influence of adverse factors, it becomes thicker and less bulky. As a result, synovial fluid is no longer able to supply the hyaline cartilage with the right amount of desired substances, causing it to rapidly dehydrate and thin. Gradually, the strength and elasticity of the cartilage decreases, the stratified regions of the fibers that form it, where cracks form, and the thickness also decreases. These changes can be noticed in the instrumental diagnostic approach, especially the narrowing of the joint space has attracted attention.
The narrowing of the joint space leads to increased friction between the bony structures that form the hip joint and increases the pressure on the already degenerated hyaline cartilage. This can cause more damage to it, affecting the function of the joint and the condition of the person, as the deformed area prevents the femoral head from sliding easily in the acetabulum. As a result, symptoms of hip joint disease appear.
If left untreated, the pathological changes will worsen and the hyaline cartilage will become more and more worn away. Subsequently, in some areas, it disappears completely, resulting in exposed bone and a dramatic increase in joint load. As the femoral head rubs directly against the bone as it moves within the acetabulum, this can cause severe pain and limited mobility. In this case, the pressure of the bone structures against each other causes bone growths to form on their surfaces.
The resulting osteophytes may have sharp parts that can damage the muscles and ligaments around the hip joint. This results in intense pain directly in the joint area and in the groin, buttocks and thighs. As a result, the patient can preserve the injured leg, reduce stress on it, and try to avoid unnecessary movement with it. This can lead to muscle wasting, further exacerbating mobility impairment and eventually leading to lameness.
reason

Hip disease can occur for many reasons, although in rare cases it occurs without any preconditions. In this case, they speak of the presence of primary or idiopathic hip arthropathy. In the vast majority of cases, secondary hip arthropathy is diagnosed as an inevitable consequence of many diseases or changes in the state of the musculoskeletal system. It can be caused by:
- Hip injuries of any nature, including fractures, dislocations, bruises, sprains, or torn ligaments;
- Heavy physical labor, professional sports, especially weightlifting, skydiving, and jumping;
- a sedentary lifestyle;
- being overweight, which can significantly increase the load on the hip joint;
- Chronic infection foci in vivo;
- Congenital deformities of the hip, such as dysplasia or dislocation;
- Metabolic and endocrine disorders, especially gout, diabetes, especially in the decompensated form;
- Aseptic necrosis of the femoral head, which may be the result of a fracture of the femoral neck, especially during conservative treatment;
- Inflammatory diseases of the joints, including rheumatoid arthritis, bursitis, tendonitis;
- spinal diseases;
- genetic susceptibility;
- The presence of bad habits, especially smoking.
Nonetheless, the main cause of hip arthropathy remains unavoidable age-related changes, the presence of which only increases the likelihood and speed of its development.
Symptoms of hip disease

The disease is characterized by gradual progression with a systemic increase in symptom intensity. Thus, in the initial stage, it may be asymptomatic or only occasionally cause anxiety in the patient, but then the condition of the hip joint deteriorates, leading to an increase in the severity of hip arthropathy symptoms until intolerable pain and significant limitation of mobility.
Thus, degenerative dystrophic changes in the hip are accompanied by:
- Pain of varying intensity, initially presenting after physical exertion or walking, and lessening with rest. Gradually, the severity of the pain syndrome increases, it occurs more frequently, lasts longer, and the time between the application of the load on the joint and the onset of pain decreases. Later, the pain persisted almost all the time, including at rest, and became unbearable. Increased pain is characteristic at any stage of disease progression during hypothermia and heavy lifting.
- Limited hip mobility, initially manifested by mild difficulty performing rotational leg movements. Over time, morning stiffness occurs and disappears after the patient "disappears". This may be accompanied by the appearance of hip edema. Movement restrictions become more pronounced and persistent as the disease progresses, that is, they do not go away after a warm-up. The patient notices a decrease in the range of motion of the legs, followed by a complete loss of the ability to perform certain movements.
- A cracked hip joint, which occurs when walking or performing physical labor, especially stretching. It becomes the result of bare bone structures rubbing against each other, accompanied by a sharp increase in pain.
- Spasms of the thigh muscles, causing diffuse pain in the thigh. This can be the result of various intra-articular disease attachments, including nerve compression, overstretching of ligaments around the joint, and the development of synovitis, an inflammation of the synovium and the accumulation of fluid in the hip joint cavity.
- Limping, first as a result of the patient's unconscious desire to unload the diseased joint and transfer the weight to the healthy leg to avoid developing or exacerbating pain, and then a muscle contracture. The latter phenomenon has occurred in the later stages of hip arthropathy, resulting in the patient's inability to fully straighten the leg and hold the leg in this position. Therefore, the lower extremity of the affected hip is always in a slightly bent position, which can cause lameness.
- The reduction in leg length, which occurs mainly in severe degenerative dystrophic changes in the hip joint, is accompanied not only by narrowing of the joint space, but also by flattening of the femoral head and muscle atrophy. As a result, the diseased leg is 1 cm or more shorter than the healthy leg.
Hip disease can affect one hip joint at the same time, or it can affect both hip joints at the same time. However, if symptoms of the disease are observed only on one side in the first case, then in the second case they are not only bilateral but also differ in intensity. It depends on how much damage each hip joint is.
Degree of hip disease
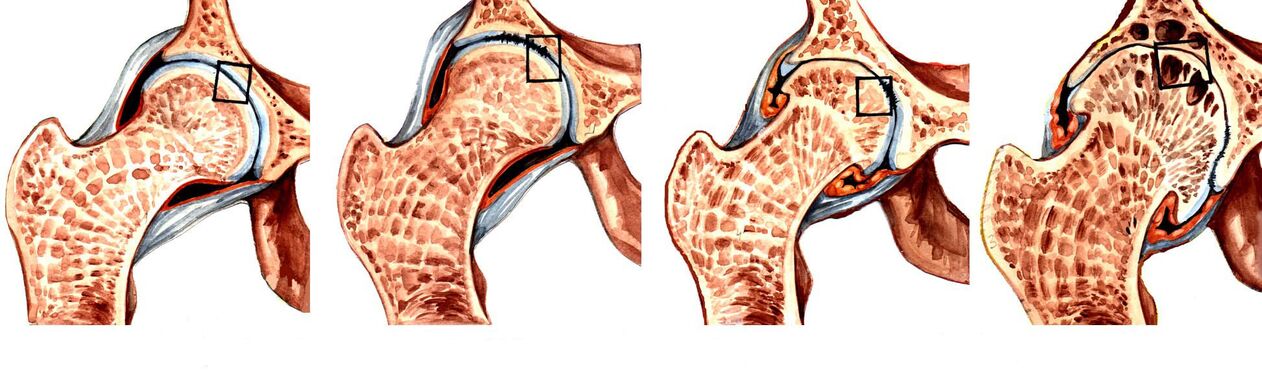
The nature of disease manifestations depends on its stage of development. There are 3 degrees of hip arthropathy in total, the first of which is considered the easiest. During the initial stages of degenerative dystrophic changes in the hip joint, only episodic pain is observed. Usually, this happens after intense physical exertion, exercise, or long walks. Therefore, patients often do not pay attention to them, attribute them to fatigue and consider them to be normal age-related changes. In this regard, first-degree hip arthropathy is diagnosed only in isolated cases, which usually occur during examinations for other causes.
As the disease progresses, its symptoms worsen and are already accompanied by what they themselves perceive as second-degree hip arthropathy. This stage of pathological development is characterized by a 50% reduction in joint space and signs of deformity with displacement of the femoral head.
As the pathology progressed further, the joint space became more narrow and the 3rd degree hip joint almost completely disappeared. This has been accompanied by the formation of multiple osteophytes. During this stage of the disease's development, the pain becomes not only intense, but also unbearable and often occurs even in a state of complete rest, including at night. As the hip joint is severely deformed, its elements can invade the nerves that pass through it, causing pain to radiate into the groin, buttocks, as well as the thighs and even the calves. It also results in the inability to move independently without the use of assistive devices such as crutches or canes.
Third-degree hip arthropathy is a direct indication for surgical treatment. If surgery is not performed on time, the femoral head fuses firmly with the acetabular surface with osteophytes. This will result in a shortened leg, with no possibility of independent movement at all, as the joint will be completely incapacitated, i. e. disabled.
diagnosis
If there are signs of hip joint disease, it is advisable to contact an orthopaedic surgeon as soon as possible. Initially, the doctor will interview the patient and find out the nature of the complaint, then examine and perform functional tests to compare the length of the legs. Often, the data obtained are sufficient to talk about the presence of hip arthropathy with a high degree of confidence.
But because this clinical presentation can accompany many other hip disorders, both inflammatory and non-inflammatory, an instrumental approach to diagnosis is required. With their help, specialists are not only able to confirm the presence of hip arthropathy, distinguish it from radiculopathy caused by spinal lesions, but also correctly assess the extent of its development, which means choosing the most effective treatment strategy.
Used today to diagnose hip disease:
- Hip X-ray - The resulting images allow you to detect signs of destructive changes, the presence of osteophytes, the nature of the deformation of the bone structure and measure the thickness of the joint space.
- CT is a more modern method of diagnosing bone pathology, providing clearer data than X-rays, but at a higher cost. Therefore, CT is prescribed in controversial cases when it is necessary to clarify the diagnosis and the degree of hip destruction.
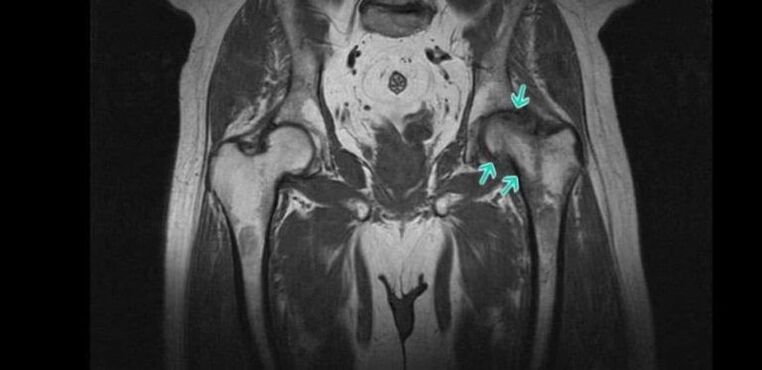
- MRI is an informative method for examining the joint, providing the greatest amount of information about the state of the joint and all its structures, especially features of the hyaline cartilage, ligaments, and blood supply.
Numerous laboratory tests are prescribed for patients, including KLA, OAM, rheumatic tests, biochemical blood tests, and more.
Conservative treatment of hip joint disease

When diagnosed as 1st or 2nd degree hip arthropathy, a conservative approach is used. For each patient, they were individually selected based on detected comorbidities. Therefore, it is necessary to consult not only an orthopedic doctor, but also a doctor of other specialties, who will choose the necessary treatments to combat the accompanying diseases.
As part of hip arthropathy treatment, patients are prescribed:
- medical treatement;
- exercise therapy;
- physiotherapy.
All patients must take steps to eliminate the influence of factors that increase the load on the legs and promote the progression of hip degenerative changes. If you are overweight, this includes adjusting your diet and increasing your level of physical activity. If the patient is regularly subjected to excessive physical exertion, he is advised to change the type of activity or reduce the training intensity if the load is due to exercise. In some cases, special bandages and orthoses are recommended to immobilize the hip joint and remove it during physical exertion.
medical treatement
As part of drug therapy, patients were individually selected for drugs taking into account existing concomitant diseases. In general, drugs from the following pharmacological groups are indicated for hip arthropathy:
- NSAIDs - a group of drugs with analgesic and anti-inflammatory properties (available in a variety of dosage forms, including tablets, capsules, gels, creams, injections, allowing you to choose the most effective and convenient applicationform);
- Corticosteroids - drugs with powerful anti-inflammatory effects, but due to the high risk of side effects, especially when using the oral form, they are only given in the form of injections for a short course of treatment;
- Muscle relaxants - drugs that help reduce muscle tone, allowing you to effectively deal with muscle spasms, commonly seen in hip disease;
- chondroprotective agents - a group of drugs that contain ingredients that the body uses to regenerate cartilage tissue;
- Preparations for improving microcirculation - help to improve the nutrition of soft tissues and activate metabolic processes in the affected area;
- B vitamins - for nerve conduction disorders due to nerve compression due to changes in the composition of the hip joint.
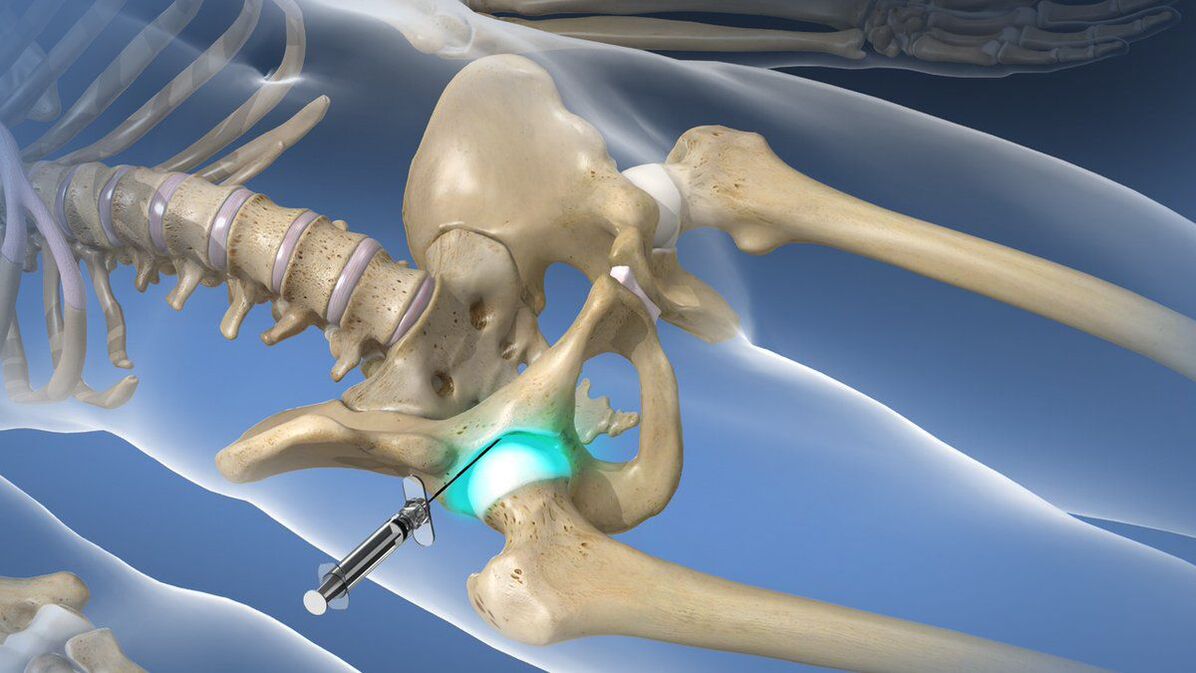
Intra- or peri-articular blocks are recommended for patients if hip disease causes acute painful episodes that cannot be stopped with the help of prescribed non-steroidal anti-inflammatory drugs. Its essence is to introduce anesthesia solution and corticosteroid directly into the hip joint cavity. This will allow you to quickly relieve pain and reduce the inflammatory process. But the lockdown can only be carried out by qualified health workers in specially prepared rooms. Such procedures are not shown to be performed at home.
exercise therapy
When diagnosing hip joint disease, regular exercise therapy must be performed. As with drug therapy, it depends on the degree of damage to the hip joint, the level of physical development of the patient, and the nature of the concomitant disease (paying particular attention to cardiovascular disease).
Thanks to daily exercise therapy, you can:
- reduce the severity of pain;
- increase the mobility of the hip joint;
- Reduce the risk of muscle wasting;
- Eliminate spasms of the thigh muscles;
- Activates blood circulation, thereby improving nutrition of affected joints.
All exercises should go smoothly, avoiding sudden movements and jerks. However, if pain develops during exercise therapy, you should definitely contact your doctor to correct the selected complex or perform a rediagnosis to rule out disease progression and the need for surgery.
physiotherapy

Comprehensive treatment of hip joint disease involves physical therapy procedures that have anti-inflammatory, analgesic, decongestant, and tonic effects on the body. Therefore, in most cases, patients will undergo 10-15 surgeries:
- ultrasound therapy;
- electrophoresis;
- UV light;
- magnetic therapy;
- laser treatment etc.
Recently, plasma lift is increasingly used as part of conservative treatment of hip arthropathy, and it can significantly increase the rate of hyaline cartilage regeneration. The essence of the procedure is to introduce purified plasma, obtained by centrifugation from the patient's own blood, into the hip joint cavity.
hip surgery

Surgical intervention is required if the patient is diagnosed with third-degree hip arthropathy, as conservative approaches are ineffective in this case. Unfortunately, this condition is very common today, as a large number of patients seek medical help when they cannot tolerate pain or have severe mobility limitations, thereby depriving them of their ability to work and move independently.
Prompt surgical intervention can completely remove these barriers, restore the patient's normal mobility, and significantly improve the quality of life. Signs of its implementation are:
- Joint space is significantly reduced by more than 80%;
- Severe pain in the hip joint that does not go away;
- Obvious mobility impairment;
- Femoral neck fracture.
The gold standard for the treatment of severe hip disease, including the elderly, is hip replacement. The procedure involves replacing a damaged hip joint with an artificial endoprosthesis made of durable and at the same time biocompatible materials. An endoprosthesis allows you to fully restore the function of your hip joint, eliminate pain and allow you to return to a mature, active life.
The essence of this surgical intervention is the removal of a small fragment of the femoral head and its neck. In addition, the surgeon needs to prepare the acetabular surface for the installation of the endoprosthesis, i. e. to remove all formed osteophytes and restore the maximum normal shape. Afterwards, the selected type of endoprosthesis is installed, fixed with special cement (preferably for the treatment of the elderly) or non-cemented. In the latter case, the endoprosthesis has a special spongy part that is in contact with the bone structure. Its fixation in the acetabulum is provided by spongy sprouted bone tissue.
The type of arthroplasty is chosen individually for each patient. The most effective is total joint replacement, which involves completely replacing the entire hip joint, the neck and head of the femur, and the acetabulum.
If the patient retains normal hyaline cartilage on the surface of the acetabulum, he can undergo partial arthroplasty, replacing only the femoral head and/or the femoral head. For this purpose, endoprostheses of different designs are used: monopolar and bipolar.
The only disadvantage of arthroplasty is the need to replace the installed endoprosthesis after 15-30 years.
After the endoprosthesis is replaced, the patient undergoes rehabilitation, the duration of which depends on the speed of tissue repair. As part of the recovery, exercise therapy, physiotherapy and therapeutic massage are prescribed.
Before the advent of modern endoprostheses, osteotomies or arthrodesis were performed in patients with grade 3 hip arthropathy. Today, these techniques are used less and less because they have many disadvantages. Therefore, arthrodesis involves fixing the bony structure of the hip joint with metal plates. As a result, the pain syndrome is completely eliminated, but the joint is completely incapacitated. Therefore, after arthrodesis, the patient can only stand but is no longer able to walk independently due to lack of movement in the hip joint. Therefore, arthrodesis is not actually performed today.
Osteotomy involves performing an artificial fracture of the femur, where the combination of bone fragments will reduce the load on the affected hip joint. However, the surgery only produces short-term effects, and joint replacements will still be required in the future.
Therefore, hip osteoarthritis is a rather dangerous disease that can lead to disability. It severely reduces the quality of life and deprives a person of the ability to work. But if you pay attention to the early signs of pathology and follow the advice of your orthopaedic surgeon, you can slow its progression and achieve significant improvements in well-being. But for hip disease that has already occurred, there can only be one solution - arthroplasty. Fortunately, this approach can be used even with severe degenerative dystrophic changes and fully restore normal hip function.